Most people over 50 years old ignore their doctor’s advice and forgo the standard, invasive test that screens for colorectal cancer and precancerous growths. Fortunately, a computer-based, noninvasive alternative to the conventional optical colonoscopy, known as virtual colonoscopy, is changing people’s attitudes—and could save tens of thousands of lives each year.
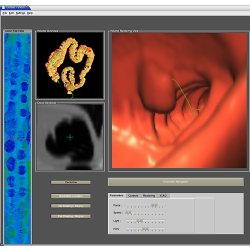
A virtual colonoscopy starts with computed tomography (CT), a common diagnostic technology that uses X-rays to record cross-sectional, 2D images of the body’s interior. A 3D model is constructed by segmenting the colon from the rest of the abdomen and using an electronic cleansing algorithm to factor out fecal material. Next, doctors use visualization software to navigate a virtual fly-through of the colon. If a polyp or suspicious growth is found, doctors can perform a virtual biopsy and investigate further.
The case for a convenient mass-screening method is strong, says Arie Kaufman, chair of the computer science department at New York’s Stony Brook University. Colorectal cancer is the third most common cancer and the second leading cause of cancer deaths in the U.S., with more than 140,000 new cases and more than 50,000 deaths a year. “If all patients 50 years of age and older will participate in these screening programs, over 92% of colorectal cancer will be prevented and over 600,000 lives could be saved worldwide every year,” Kaufman says.
Virtual colonoscopies became possible in the mid-1990s, when Kaufman and others developed volume-rendering techniques that enabled 3D, virtual fly-throughs and associated tools, which were soon commercialized.
Virtual colonoscopies have recently earned the imprimatur of the medical establishment, which prefers the formal term CT colonography. In a study at U.S. military hospitals, 1,233 symptomless subjects underwent a virtual colonoscopy, followed by a conventional optical colonoscopy, on the same day. The virtual colonoscopy results, reported in the New England Journal of Medicine in 2003, showed 94% sensitivity (real polyps found) and 96% specificity (false-positive rate) for polyps 8mm and largernumbers comparable to those of optical colonoscopy, the gold standard among doctors. Subsequently, the U.S. Food and Drug Administration approved virtual colonoscopy for colon cancer screening.
Virtual colonoscopy outperforms optical colonoscopy in certain ways, advocates claim. A University of Wisconsin study, for example, found it better at finding 8mm and 10mm polyps. It also outperforms optical colonoscopy in finding polyps hidden in folds and around corners of the twisting tube of the colon, and in reliably reaching the farthest reaches, called the caecum. It can also do something optical colonoscopy, by its nature, cannot do: spot polyps on the colon’s outer walls.
Also, because it is noninvasive, a virtual colonoscopy avoids the risk of the rare but deadly tears or holes that can occur during an optical colonoscopy (and which can require immediate surgery). “The examination is done on the data, rather than the patient,” says Dr. C. Daniel Johnson, a principal investigator at the Mayo Clinic in Scottsdale, AZ, and the lead researcher on several studies.
Virtual colonoscopy’s only significant health risk is a patient’s exposure to radiation. This trade-off is being addressed in a technique called low dose, which Kaufman’s group is researching, with a grant from the National Institutes of Health (NIH). Another drawback of a virtual colonoscopy is it can’t remove polyps; patients still need an optical colonoscopy for their surgical excision. However, a virtual colonoscopy study has shown that only about 7% of patients required such follow-up.
Insurers, however, have been slow to catch on. Medicare, for example, announced a tentative decision earlier this year to not pay for virtual colonoscopies. And some insurers have setup the payment codes that healthcare providers need to be reimbursed for the procedure, but the money has yet to materialize. However, Kaufman says the political will to mandate coverage is growing, and patients can pressure their insurer to pay for a virtual colonoscopy by refusing to undergo optical colonoscopy.
Early Detection
Screening is critical because a patient’s successful outcome often hinges on the early detection of polyps. A virtual colonoscopy removes many of the uncomfortable hurdles. “Only 15%19% of individuals eligible for screening currently undergo colon evaluation,” says Hiroyuki Yoshida, an associate professor at Harvard Medical School and director of 3D Imaging Research at Massachusetts General Hospital. “The cathartic cleansing required for bowel preparation is the biggest barrier.”
A virtual colonoscopy still requires preparation, so developing a laxative-free procedure will be indispensable to its practicality, Yoshida says. One hitch: eliminating laxatives leaves more fecal matter in the colon, which requires improvements in electronic cleansing. What’s more, patients still must ingest an oral contrast agent, such as barium or iodine, and air or carbon dioxide must still be used to distend the colon. Yet, a laxative-free virtual colonoscopy could be ready for public use in the near future, Yoshida says.
Many of the challenging issues with virtual colonoscopies involve software applications. Computer-aided detection (CAD), the focus of Yoshida’s research, brings much-needed automation to electronic cleansing and polyp detection. It holds great promise, says Kaufman. “In mammography, this has been entirely successful,” he notes. “Basically, the computer is another set of eyes.”
Virtual colonoscopies could become more available in remote places via telemedicine.
Skill in interpreting diagnostic images varies among radiologists, who can mistake the colon’s normal valves and folds for polyps. Yoshida says CAD could make results more objective and consistent, and shorten radiologists’ learning curve. It could also be useful in hospitals that lack expertise with virtual colonoscopies.
However, CAD presents its own challenges. “Sometimes CAD’s weak spots are comparable to human viewers’ weak spots,” says Dr. Ronald Summers, a radiologist and senior investigator at NIH. One important challenge is detecting flat lesions, which are more difficult to detect with a virtual or optical colonoscopy, but constitute a higher risk for cancer.
Kaufman has co-developed a novel CAD technique, utilizing colon flattening and volume rendering, which has achieved perfect sensitivity and tolerable specificity, and could function as either a first or second reader.
Another problem is false positives: they require patients to undergo an optical colonoscopy. Of course, false positives aren’t as deadly as false negatives, and doctors can dismiss false positives with a second read. Ideally, Kaufman says, CAD should be a first reader for radiologists, who can inspect the regions flagged by it. “I think the second read is the one the radiologist should use, because it has the highest sensitivity, but we’re still working that out,” Dr. Summers says.
There is also considerable debate on how to best combine 2D and 3D imagery. “We seem to be moving to a consensus that the sensitivity and specificity of 2D and 3D are comparable,” Dr. Summers says. “The question is which one do you use as your primary.” Yoshida thinks CAD could soon replace 3D visual fly-throughs for first reads, though expert examination of 2D images—what radiologists called “problem solving”—will still be needed.
2D is important in a virtual biopsy, which depends on flattening the images to simulate what pathologists do when dissecting a polyp. “They will slice it along its length and lay it flat and look at it,” Dr. Summers says. “You do the same thing on the computer.” Some experts, he notes, think such 2D dissection provides faster diagnosing than 3D fly-through.
Seeking Improvements
Medical and computer-science researchers are striving to make virtual colonoscopy technology more accurate, affordable, easier to use, and patient friendly.
A technique called dual-energy imaging, for instance, highlights polyps by blending images derived from different radiation doses to increase contrast, Yoshida says. And graphics processing unit-based rendering is being touted as a faster method of getting images to radiologists, as Kaufman’s group has done. Also, Dr. Summers says his collaborators and him have figured out how to bolster CAD with wavelets on manifolds to reduce false positives by more precisely characterizing polyps. And machine learning and neural nets are the subject of ongoing research.
“The examination is done on the data, rather than the patient,” says Dr. c. Daniel Johnson.
To increase virtual colonoscopies’ usability, computer scientists are also focusing attention on the PCs that are used for analyzing images. One possibility is off-site image processing, which Yoshida says Massachusetts General Hospital is ready to implement.
Others hope to democratize virtual colonoscopies by getting the software to run effectively on desktop and laptop computers. For example, the Redmond, WA, company FiatLux Imaging employs the Direct3D technology in video games and in virtual colonoscopies. “It’s usually required to run on very heavy-duty, expensive hardware,” says Rosemary Fisher, FiatLux’s clinical application specialist. “That is prohibitively expensive for small hospitals and clinics.” Many of them lack colonography software and have little financial incentive to invest in it before insurers start uniformly reimbursing for virtual colonoscopies. But as spiral CT scanners become more broadly distributed, affordable volume-rendering software, such as FiatLux’s Visualize, might make virtual colonoscopies more available in remote places via telemedicine.
The takeaway message is that virtual colonoscopies are poised to dramatically increase successful colon screening outcomes. Says Kaufman, “We’re going to save 50,000 lives every year just in the U.S.”




{kind=link}
Join the Discussion (0)
Become a Member or Sign In to Post a Comment